Fallen Arches Explained
Overview

When standing, most people have a gap under the arch of their foot. Flat feet, or pes planus is the term used to describe collapsed arches, meaning that the entire sole of the foot rests partially or completely on the ground. A simple way to check to see if you have flat feet is to wet your feet and step onto a dry, flat surface. Step away from your footprint; if you see a complete footprint, you more than likely have flat feet. If you only see toes, the pads of your feet, and your heels, you probably do not have flat feet. People who have flat feet usually roll their feet over to the inner side when they walk. The feet may even appear to point outward because of this movement. In most cases, the condition cannot be prevented.
Causes
Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum.
Symptoms
Structural problems in your feet like fallen arches can alter your walking pattern, running pattern and cause pain throughout your body. Clear and accurate assessment of the mechanics of your lower limbs is key to understanding the profound effect that subtle faults in your foot, ankle, knee and hip alignment can cause.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks.
pes planus orthotics
Non Surgical Treatment
There are different modalities of treatment that are available to manage flat feet and fallen arches. The type of treatment that is chosen depends upon how severe the condition is and what symptoms the patients are experiencing. Below is a brief description of the available treatment modalities. In the event that the patient is experiencing swelling of the feet, rest and ice application is usually the initial treatment step. Oral anti-inflammatories may be offered which can help reduce inflammation as well as associated pain. Physical therapy has good outcomes and can include different exercises such as stretches and strengthening of the surrounding muscles. Changes in footwear and activity modification are also important when dealing with a painful flat (pronated) foot. These days, orthotic insoles are easily available either over the counter or through your Podiatrist which can effectively help maintain the arch of the foot and reduce the amount of stress placed on the foot. Podiatrists are able to prescribe a variety of different devices from prefabricated to customized and are trained to determine the most appropriate device for each individual. In order to offer the right kind of orthotic insole, podiatrists may perform a test called gait analysis. This involves asking the patient to walk and videoing the different movements that the foot of forms during the walking. Features such as over pronation can be easily seen on this and orthotic insoles can be prescribed to correct the specific abnormalities that are picked up on this analysis. Overall, orthotic treatment can result in a significant improvement in foot movement and reduction in foot discomfort.
Surgical Treatment

In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Prevention
oll away pain. If you're feeling pain in the arch area, you can get some relief by massaging the bottom of your foot. A regular massage while you're watching TV can do wonders" Stretch out. Doing the same type of stretching exercises that runners do in their warm-up can help reduce arch pain caused by a tight heel cord. One of the best exercises is to stand about three feet from a wall and place your hands on the wall. Leaning toward the wall, bring one foot forward and bend the knee so that the calf muscles of the other leg stretch. Then switch legs. Stretching is particularly important for women who spend all week in heels and then wear exercise shoes or sneakers on weekends. Get measured each time you buy new shoes. Don't assume that since you always wore a particular size, you always will. Too many people try to squeeze into their 'regular' shoe size and wind up with serious foot problems or sores on their feet. When your arch is falling, your feet may get longer or wider and you may or may not feel pain, so getting your foot measured each time you buy shoes is a good indicator of your arch's degeneration. Examine your shoes. If the heel is worn down, replace it. But if the back portion of the shoe is distorted or bent to one side, get yourself into a new pair of supportive shoes like those made specifically for walking. That's because flat feet can affect your walking stride, and failing to replace worn shoes may lead to knee or hip pain.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
When standing, most people have a gap under the arch of their foot. Flat feet, or pes planus is the term used to describe collapsed arches, meaning that the entire sole of the foot rests partially or completely on the ground. A simple way to check to see if you have flat feet is to wet your feet and step onto a dry, flat surface. Step away from your footprint; if you see a complete footprint, you more than likely have flat feet. If you only see toes, the pads of your feet, and your heels, you probably do not have flat feet. People who have flat feet usually roll their feet over to the inner side when they walk. The feet may even appear to point outward because of this movement. In most cases, the condition cannot be prevented.
Causes
Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum.
Symptoms
Structural problems in your feet like fallen arches can alter your walking pattern, running pattern and cause pain throughout your body. Clear and accurate assessment of the mechanics of your lower limbs is key to understanding the profound effect that subtle faults in your foot, ankle, knee and hip alignment can cause.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks.
pes planus orthotics
Non Surgical Treatment
There are different modalities of treatment that are available to manage flat feet and fallen arches. The type of treatment that is chosen depends upon how severe the condition is and what symptoms the patients are experiencing. Below is a brief description of the available treatment modalities. In the event that the patient is experiencing swelling of the feet, rest and ice application is usually the initial treatment step. Oral anti-inflammatories may be offered which can help reduce inflammation as well as associated pain. Physical therapy has good outcomes and can include different exercises such as stretches and strengthening of the surrounding muscles. Changes in footwear and activity modification are also important when dealing with a painful flat (pronated) foot. These days, orthotic insoles are easily available either over the counter or through your Podiatrist which can effectively help maintain the arch of the foot and reduce the amount of stress placed on the foot. Podiatrists are able to prescribe a variety of different devices from prefabricated to customized and are trained to determine the most appropriate device for each individual. In order to offer the right kind of orthotic insole, podiatrists may perform a test called gait analysis. This involves asking the patient to walk and videoing the different movements that the foot of forms during the walking. Features such as over pronation can be easily seen on this and orthotic insoles can be prescribed to correct the specific abnormalities that are picked up on this analysis. Overall, orthotic treatment can result in a significant improvement in foot movement and reduction in foot discomfort.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Prevention
oll away pain. If you're feeling pain in the arch area, you can get some relief by massaging the bottom of your foot. A regular massage while you're watching TV can do wonders" Stretch out. Doing the same type of stretching exercises that runners do in their warm-up can help reduce arch pain caused by a tight heel cord. One of the best exercises is to stand about three feet from a wall and place your hands on the wall. Leaning toward the wall, bring one foot forward and bend the knee so that the calf muscles of the other leg stretch. Then switch legs. Stretching is particularly important for women who spend all week in heels and then wear exercise shoes or sneakers on weekends. Get measured each time you buy new shoes. Don't assume that since you always wore a particular size, you always will. Too many people try to squeeze into their 'regular' shoe size and wind up with serious foot problems or sores on their feet. When your arch is falling, your feet may get longer or wider and you may or may not feel pain, so getting your foot measured each time you buy shoes is a good indicator of your arch's degeneration. Examine your shoes. If the heel is worn down, replace it. But if the back portion of the shoe is distorted or bent to one side, get yourself into a new pair of supportive shoes like those made specifically for walking. That's because flat feet can affect your walking stride, and failing to replace worn shoes may lead to knee or hip pain.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Surgery To Correct Leg Length Discrepancy
Overview
Leg length discrepancy, or as it has been alternatively termed, the short leg syndrome, is by far the most important postural asymmetry. Limb length discrepancy is simply defined as a condition where one leg is shorter than the other. If a substantial difference exists, disruptive effects on gait and posture can occur. Leg length discrepancy can be divided into two etiological groups. Structural. True shortening of the skeleton from congenital, traumatic or diseased origins. Functional. Development from altered mechanics of the lower body, such as foot hyperpronation or supination, pelvic obliquity, muscle/joint imbalances, poor trunk stabilization and deep fascial strain patterns.
Causes
Some limb-length differences are caused by actual anatomic differences from one side to the other (referred to as structural causes). The femur is longer (or shorter) or the cartilage between the femur and tibia is thicker (or thinner) on one side. There could be actual deformities in one femur or hip joint contributing to leg length differences from side to side. Even a small structural difference can amount to significant changes in the anatomy of the limb. A past history of leg fracture, developmental hip dysplasia, slipped capital femoral epiphysis (SCFE), short neck of the femur, or coxa vara can also lead to placement of the femoral head in the hip socket that is offset. The end-result can be a limb-length difference and early degenerative arthritis of the hip.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).

what shoes make you taller
Surgical Treatment
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Leg length discrepancy, or as it has been alternatively termed, the short leg syndrome, is by far the most important postural asymmetry. Limb length discrepancy is simply defined as a condition where one leg is shorter than the other. If a substantial difference exists, disruptive effects on gait and posture can occur. Leg length discrepancy can be divided into two etiological groups. Structural. True shortening of the skeleton from congenital, traumatic or diseased origins. Functional. Development from altered mechanics of the lower body, such as foot hyperpronation or supination, pelvic obliquity, muscle/joint imbalances, poor trunk stabilization and deep fascial strain patterns.
Causes
Some limb-length differences are caused by actual anatomic differences from one side to the other (referred to as structural causes). The femur is longer (or shorter) or the cartilage between the femur and tibia is thicker (or thinner) on one side. There could be actual deformities in one femur or hip joint contributing to leg length differences from side to side. Even a small structural difference can amount to significant changes in the anatomy of the limb. A past history of leg fracture, developmental hip dysplasia, slipped capital femoral epiphysis (SCFE), short neck of the femur, or coxa vara can also lead to placement of the femoral head in the hip socket that is offset. The end-result can be a limb-length difference and early degenerative arthritis of the hip.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).
what shoes make you taller
Surgical Treatment
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Heel Soreness
Overview
The most common cause of heel pain is plantar fasciitis. Many patients with plantar fasciitis have a heel spur on the front and bottom of their heel, but heel spurs do not cause pain. The common name is "heel spur" because it's easier to pronounce than "plantar fasciitis" and doctors are able to point to the spur on an x-ray. Causes of heel pain include inadequate flexibility in the calf muscles, lack of arch support, being overweight, suddenly increasing activity, and spending too much time on the feet. Arch support was rated the best treatment in our first survey of 1,800 visitors to heelspurs.com. The Plantar Fasciitis Orthotic is getting the best customer reviews and it is the most popular product. It is new for 2011. Returning customers may be seeking the Pinnacle Orthotic. The primary difference is that the PF Orthotic should be used only for current cases of plantar fasciitis or heel spurs and the Pinnacle is best for general use once the condition has subsided. Survery respondents also benefited from: rest, ice, tape, and night splints.
Causes
There are many possible causes of heel pain. Most commonly it is a chronic, long-term pain that results of some type of faulty biomechanics (abnormalities in the way you walk) that place too much stress on the heel bone and the soft tissues that attach to it. Chronic pain is a common result of standing or walking too many hours in the course of a day, working on concrete, being overweight, wearing poorly-constructed shoes, having an overly-pronated foot type (where the arch collapses excessively) or the opposite--having too high an arch. Women seem to get this slightly more often than men, and while any age can be affected, it usually occurs between 30 and 50 years of age. The other type of heel pain is the sort you get from an acute injury--a bruise to the bone or soft tissue strain resulting from a strenuous activity, like walking, running, or jumping, or from some degree of trauma. While there are dozens of possible causes to heel pain, I will review some of the more common causes. Arch Pain/Plantar Fasciitis. One of those often-painful soft tissue that attaches to heel spurs at the bottom of the foot is called "plantar fascia". Fascia, located throughout the body, is a fibrous connective tissue similar to a ligament. You can see fascia as some of that white, connective tissue attaching to bones, when you pull apart meat. The "plantar" fascia in our bodies is that fascia which is seen on the bottom (or plantar portion) of the foot, extending from the heel bone to the ball of the foot. Compared to other fascia around the body, plantar fascia is very thick and very strong. It has to be strong because of the tremendous amount of force it must endure when you walk, run or jump. But while the plantar fascia is a strong structure, it can still get injured, most commonly when it is stretched beyond its normal length over long periods of time. Plantar Fascitis. When plantar fascia is injured, the condition is called "plantar fasciitis", pronounced "plan-tar fash-I-tis". (Adding "-itis" to the end of a word means that structure is inflamed.) It is sometimes known more simply as 'fasciitis'. Plantar fasciitis is the most common type of arch pain. Symptoms of plantar fasciitis may occur anywhere along the arch, but it is most common near its attachment to the heel bone.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
deelsonheels
Prevention

Wear properly fitting shoes. Place insoles or inserts in your shoes to help control abnormal foot motion. Maintain a healthy weight. Exercise and do foot stretches as they have been shown to decrease the incidence of heel pain.
The most common cause of heel pain is plantar fasciitis. Many patients with plantar fasciitis have a heel spur on the front and bottom of their heel, but heel spurs do not cause pain. The common name is "heel spur" because it's easier to pronounce than "plantar fasciitis" and doctors are able to point to the spur on an x-ray. Causes of heel pain include inadequate flexibility in the calf muscles, lack of arch support, being overweight, suddenly increasing activity, and spending too much time on the feet. Arch support was rated the best treatment in our first survey of 1,800 visitors to heelspurs.com. The Plantar Fasciitis Orthotic is getting the best customer reviews and it is the most popular product. It is new for 2011. Returning customers may be seeking the Pinnacle Orthotic. The primary difference is that the PF Orthotic should be used only for current cases of plantar fasciitis or heel spurs and the Pinnacle is best for general use once the condition has subsided. Survery respondents also benefited from: rest, ice, tape, and night splints.
Causes
There are many possible causes of heel pain. Most commonly it is a chronic, long-term pain that results of some type of faulty biomechanics (abnormalities in the way you walk) that place too much stress on the heel bone and the soft tissues that attach to it. Chronic pain is a common result of standing or walking too many hours in the course of a day, working on concrete, being overweight, wearing poorly-constructed shoes, having an overly-pronated foot type (where the arch collapses excessively) or the opposite--having too high an arch. Women seem to get this slightly more often than men, and while any age can be affected, it usually occurs between 30 and 50 years of age. The other type of heel pain is the sort you get from an acute injury--a bruise to the bone or soft tissue strain resulting from a strenuous activity, like walking, running, or jumping, or from some degree of trauma. While there are dozens of possible causes to heel pain, I will review some of the more common causes. Arch Pain/Plantar Fasciitis. One of those often-painful soft tissue that attaches to heel spurs at the bottom of the foot is called "plantar fascia". Fascia, located throughout the body, is a fibrous connective tissue similar to a ligament. You can see fascia as some of that white, connective tissue attaching to bones, when you pull apart meat. The "plantar" fascia in our bodies is that fascia which is seen on the bottom (or plantar portion) of the foot, extending from the heel bone to the ball of the foot. Compared to other fascia around the body, plantar fascia is very thick and very strong. It has to be strong because of the tremendous amount of force it must endure when you walk, run or jump. But while the plantar fascia is a strong structure, it can still get injured, most commonly when it is stretched beyond its normal length over long periods of time. Plantar Fascitis. When plantar fascia is injured, the condition is called "plantar fasciitis", pronounced "plan-tar fash-I-tis". (Adding "-itis" to the end of a word means that structure is inflamed.) It is sometimes known more simply as 'fasciitis'. Plantar fasciitis is the most common type of arch pain. Symptoms of plantar fasciitis may occur anywhere along the arch, but it is most common near its attachment to the heel bone.
Symptoms
Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
deelsonheels
Prevention
Wear properly fitting shoes. Place insoles or inserts in your shoes to help control abnormal foot motion. Maintain a healthy weight. Exercise and do foot stretches as they have been shown to decrease the incidence of heel pain.
Combating Mortons Neuroma
Overview
 This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton.
This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton.
Causes
Poorly fitted footwear can be a cause. Shoes that have a tight and narrow toe box can cause the never to become entrapped causing the pain. High heeled shoes abnormally place the metatarsals under extreme pressure which can cause Morton?s Neuroma. In cases of abnormal pronation, there can be significant motion between the 3rd and 4th metatarsals which can cause an irritation to the nerve that runs between them. This inflammation causes the pain.
Symptoms
A Morton's neuroma usually causes burning pain, numbness or tingling at the base of the third, fourth or second toes. Pain also can spread from the ball of the foot out to the tips of the toes. In some cases, there also is the sensation of a lump, a fold of sock or a "hot pebble" between the toes. Typically, the pain of a Morton's neuroma is relieved temporarily by taking off your shoes, flexing your toes and rubbing your feet. Symptoms may be aggravated by standing for prolonged periods or by wearing high heels or shoes with a narrow toe box.
Diagnosis
Based on the physical examination, your doctor usually can diagnose a Morton's neuroma without additional testing. A foot X-ray may be ordered to make sure that there isn't a stress fracture, but it will not show the actual neuroma. If the diagnosis is in doubt, your doctor may request magnetic resonance imaging (MRI) of the foot.
Non Surgical Treatment
Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.
Surgical Treatment
Operative treatment of Morton?s neuroma should be entertained only after failure of non-operative management. Standard operative treatment involves identifying the nerve and cutting (resecting) it proximal to the point where it is irritated/injured. This is usually done through an incision on the top (dorsal) aspect of the foot, although an incision on the sole (plantar) aspect of the foot can be used. Some physicians will attempt to treat Morton?s neuroma by releasing the intermetatarsal ligament, and freeing the nerve of local scar tissue. This may also be beneficial.
This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton.Causes
Poorly fitted footwear can be a cause. Shoes that have a tight and narrow toe box can cause the never to become entrapped causing the pain. High heeled shoes abnormally place the metatarsals under extreme pressure which can cause Morton?s Neuroma. In cases of abnormal pronation, there can be significant motion between the 3rd and 4th metatarsals which can cause an irritation to the nerve that runs between them. This inflammation causes the pain.
Symptoms
A Morton's neuroma usually causes burning pain, numbness or tingling at the base of the third, fourth or second toes. Pain also can spread from the ball of the foot out to the tips of the toes. In some cases, there also is the sensation of a lump, a fold of sock or a "hot pebble" between the toes. Typically, the pain of a Morton's neuroma is relieved temporarily by taking off your shoes, flexing your toes and rubbing your feet. Symptoms may be aggravated by standing for prolonged periods or by wearing high heels or shoes with a narrow toe box.
Diagnosis
Based on the physical examination, your doctor usually can diagnose a Morton's neuroma without additional testing. A foot X-ray may be ordered to make sure that there isn't a stress fracture, but it will not show the actual neuroma. If the diagnosis is in doubt, your doctor may request magnetic resonance imaging (MRI) of the foot.
Non Surgical Treatment
Common treatments involve wearing different shoes or using arch supports. Resting the foot, massaging the toes and using an ice pack may work for some people. A GP or a podiatrist (foot specialist) may also recommend anti-inflammatory painkillers or a course of steroid injections. Numbing injections, in which alcohol and a local anaesthetic are injected into the affected area of the foot, may also be effective. In extreme cases, when the condition does not respond to treatment, day case surgery may be needed.
Surgical Treatment
Operative treatment of Morton?s neuroma should be entertained only after failure of non-operative management. Standard operative treatment involves identifying the nerve and cutting (resecting) it proximal to the point where it is irritated/injured. This is usually done through an incision on the top (dorsal) aspect of the foot, although an incision on the sole (plantar) aspect of the foot can be used. Some physicians will attempt to treat Morton?s neuroma by releasing the intermetatarsal ligament, and freeing the nerve of local scar tissue. This may also be beneficial.
Leg Length Discrepancy And Shoe Lifts
There are not one but two unique variations of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter compared to the other. Through developmental stages of aging, the human brain senses the walking pattern and identifies some difference. The entire body typically adapts by dipping one shoulder over to the "short" side. A difference of less than a quarter inch is not grossly excessive, doesn't need Shoe Lifts to compensate and generally doesn't have a profound effect over a lifetime.

Leg length inequality goes mainly undiagnosed on a daily basis, however this issue is easily corrected, and can eradicate many incidents of low back pain.
Treatment for leg length inequality usually consists of Shoe Lifts. These are affordable, often costing under twenty dollars, compared to a custom orthotic of $200 if not more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is the most common ailment affecting men and women today. Over 80 million men and women have problems with back pain at some stage in their life. It is a problem which costs businesses huge amounts of money each year on account of lost time and productivity. Fresh and superior treatment methods are continually sought after in the hope of minimizing the economic impact this issue causes.

People from all corners of the earth suffer from foot ache due to leg length discrepancy. In these types of cases Shoe Lifts can be of very helpful. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by countless experienced orthopaedic practitioners".
So that they can support the body in a well balanced manner, your feet have a crucial role to play. Despite that, it can be the most overlooked area of the human body. Many people have flat-feet meaning there is unequal force placed on the feet. This causes other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts make sure that correct posture and balance are restored.
Leg length inequality goes mainly undiagnosed on a daily basis, however this issue is easily corrected, and can eradicate many incidents of low back pain.
Treatment for leg length inequality usually consists of Shoe Lifts. These are affordable, often costing under twenty dollars, compared to a custom orthotic of $200 if not more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is the most common ailment affecting men and women today. Over 80 million men and women have problems with back pain at some stage in their life. It is a problem which costs businesses huge amounts of money each year on account of lost time and productivity. Fresh and superior treatment methods are continually sought after in the hope of minimizing the economic impact this issue causes.
People from all corners of the earth suffer from foot ache due to leg length discrepancy. In these types of cases Shoe Lifts can be of very helpful. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by countless experienced orthopaedic practitioners".
So that they can support the body in a well balanced manner, your feet have a crucial role to play. Despite that, it can be the most overlooked area of the human body. Many people have flat-feet meaning there is unequal force placed on the feet. This causes other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts make sure that correct posture and balance are restored.
Learn How To Protect Against Posterior Calcaneal Spur

Overview
Heel Spurs should be called a traction spurs because they grow in the same direction that the tendons pull away from the heel bone, which is why it can occur on the bottom of the heel (Plantar Fasciitis) and on the back of the heel (Achilles Tendonitis). Some patients may only develop one type of heel spur, but both these problems are closely related so it's not unusual for a patient to have both heel spurs. It's important to note though that most heel spurs aren't the cause of your heel pain.
Causes
At the onset of this condition, pain and swelling become present, with discomfort particularly noted as pushing off with the toes occurs during walking. This movement of the foot stretches the fascia that is already irritated and inflamed. If this condition is allowed to continue, pain is noticed around the heel region because of the newly formed bone, in response to the stress. This results in the development of the heel spur. It is common among athletes and others who run and jump a significant amount.

Symptoms
The vast majority of people who have heel spurs feel the asscociated pain during their first steps in the morning. The pain is quite intense and felt either the bottom or front of the heel bone. Typically, the sharp pain diminishes after being up for a while but continues as a dull ache. The pain characteristically returns when first standing up after sitting for long periods.
Diagnosis
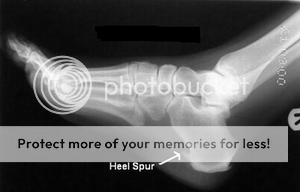
Heel spurs and plantar fasciitis is usually diagnosed by your physiotherapist or sports doctor based on your symptoms, history and clinical examination. After confirming your heel spur or plantar fasciitis they will investigate WHY you are likely to be predisposed to heel spurs and develop a treatment plan to decrease your chance of future bouts. X-rays will show calcification or bone within the plantar fascia or at its insertion into the calcaneus. This is known as a calcaneal or heel spur. Ultrasound scans and MRI are used to identify any plantar fasciitis tears, inflammation or calcification. Pathology tests may identify spondyloarthritis, which can cause symptoms similar to plantar fasciitis.
Non Surgical Treatment
The first line of treatment for Heel Spur is to avoid the activities and positions that cause the pain. A physician can evaluate your foot with an X-ray to diagnose Heel Spur and determine a course of treatment. This condition can often be treated by non-surgical means; however in severe cases surgery may be necessary to relieve the pain. The most common surgical procedures treat the soft tissues around the Heel Spur, often a tarsal tunnel release or a plantar fascia release. Injections for heel spurs are sometimes controversial as steroids may cause heel pad atrophy or damage the plantar fascia.
Surgical Treatment
When chronic heel pain fails to respond to conservative treatment, surgical treatment may be necessary. Heel surgery can provide pain relief and restore mobility. The type of procedure used is based on examination and usually consists of releasing the excessive tightness of the plantar fascia, called a plantar fascia release. The procedure may also include removal of heel spurs.
Prevention
You can prevent heel spurs by wearing well-fitting shoes with shock-absorbent soles, rigid shanks, and supportive heel counters; choosing appropriate shoes for each physical activity; warming up and doing stretching exercises before each activity; and pacing yourself during the activities. Avoid wearing shoes with excessive wear on the heels and soles. If you are overweight, losing weight may also help prevent heel spurs.
What Can Induce Posterior Calcaneal Spur

Overview
Heel spur is a thorn-like, bony protrusion of the heel bone, which can become inflamed through irritation, thus causing pain. A heel spur forms at the tendon attachments on the muscles of the heel bone as a result of micro-injuries to the tissue caused by overstraining. As part of the healing process for these micro-injuries, the body stores bone material in the tendon attachments as a repair mechanism. Heel spurs can develop over a very long period without causing major complaints. However, irritation of the area surrounding the ossified tendon attachment can cause inflammations. Left untreated, the inflammations can in turn lead to increased ossification and thus to permanent degradation with a risk of chronic manifestation. The normal rolling procedure that we all use when walking is then frequently no longer possible.
Causes
Heel spurs form in some patients who have plantar fasciitis (PLAN-tar fash-ee-I-tis), and tend to occur in patients who have had the problem for a prolonged period of time. While about 70 percent of patients with plantar fasciitis have a heel spur, X-rays also show about 50 percent of patients with no symptoms of plantar fasciitis also have a heel spur.
Symptoms
Heel spurs result in a jabbing or aching sensation on or under the heel bone. The pain is often worst when you first arise in the morning and get to your feet. You may also experience pain when standing up after prolonged periods of sitting, such as work sessions at a desk or car rides. The discomfort may lessen after you spend several minutes walking, only to return later. Heel spurs can cause intermittent or chronic pain.
Diagnosis
Heel spurs and plantar fasciitis is usually diagnosed by your physiotherapist or sports doctor based on your symptoms, history and clinical examination. After confirming your heel spur or plantar fasciitis they will investigate WHY you are likely to be predisposed to heel spurs and develop a treatment plan to decrease your chance of future bouts. X-rays will show calcification or bone within the plantar fascia or at its insertion into the calcaneus. This is known as a calcaneal or heel spur. Ultrasound scans and MRI are used to identify any plantar fasciitis tears, inflammation or calcification. Pathology tests may identify spondyloarthritis, which can cause symptoms similar to plantar fasciitis.
Non Surgical Treatment
By reducing excessive motion and controlling and supporting the foot during physical activities an orthotic can help to limit how far the plantar fascia is pulled or torn away from the heel. A Heel Spur pad can be offered- which is a pad designed to take pressure off the spur. If the problem persists, consult your foot doctor.
Surgical Treatment
When chronic heel pain fails to respond to conservative treatment, surgical treatment may be necessary. Heel surgery can provide pain relief and restore mobility. The type of procedure used is based on examination and usually consists of releasing the excessive tightness of the plantar fascia, called a plantar fascia release. The procedure may also include removal of heel spurs.